
 This is the time of year when we all talk about making our resolutions for the new year. Since spoonies like us cannot resolve to "be healthy" (wouldn't that be nice!), I've come up with a list of resolutions that are applicable for those of us with chronic illness and chronic pain:
I hope that everyone is recovering nicely from however you celebrate December 25th. Just remember: 
 Here's to a holiday season filled with many, many spoons. Merry Christmas to you and yours.   Holidays are tough for those of us with chronic illnesses and pain. Typically, hours of travel, cooking, eating, mingling, and pretending that you are fine are expected. Holidays are, in short, a recipe for a pain explosion. I can usually make it through Christmas day OK, but I am suffering (i.e. stumbling from my bed to my couch is the extent of my movement) for the week following. This year, I am going to try to follow my own advice for a low-pain holiday:
 I've realized that in the past 2 years, I've withstood a ridiculous amount of medical procedures, many of which I wouldn't wish on my worst enemy (chest tube, anyone?). I've also battled with insurance companies, disability, non-believing physicians, and dubious friends, family, and co-workers. Some of these skirmishes are ongoing, some probably will always be there. But even through the frustration and the daily pain, I try to keep moving forward. I have been called a "tough cookie" many times, and I believe that living each day with chronic pain and illness has developed the resilience I now have. It makes sense that spoonies like us have to be resilient; it becomes a trait necessary to survive with chronic pain and illness. Resilience is the only way we can function and live anything close to a "normal" life. It is how we can bounce back after a hospitalization, clean the house during a flare, educate physicians, and care for others. We are spoonies, are we are resilient! 
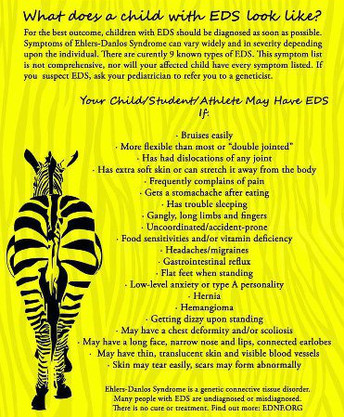 I am going to get a little personal here. I wasn't diagnosed with EDS hypermobility type until I was pushing 30. However, signs were apparent throughout my childhood. Not just small sign either, but glaring, huge red flags. However, no one ever put the pieces together. Add to this story a few more details: my family's favorite line while I was growing up was "suck it up"; sports were revered in my school and by my family; my dad is an ex-football player and coach and really wanted me to be a boy. I'm sure you can guess where this all leads--I was a major tomboy who played just about every sport and ignored every injury. I somehow always managed my numerous sports-related injuries (As a side note, I also became so used to the sports trainer's office at my high school that I was allowed to tape up other athletes). These problems were all was all considered due to my "clumsiness" or "double-jointed-ness" or just plain bad luck. Then, in my senior year in high school when spring board diving, I inexplicably dislocated my patella during a routine warm-up dive before a meet. Still, no one could figure out the underlying problem. And my family, coaches, etc. just kept pushing. I finished that season of diving, and the spring season of track and field.
I'm not a big believer in the "blame the parents for everything" theories in psychology. However, I am sure that if I hadn't been told to "suck it up" so much as a child, and listened to such advice, my joints would be better today. I probably wouldn't be dislocating at the rate I am now. I surely wouldn't have the insane amounts of scar tissue and other "floaters" that I do in my joints. I'm obviously not blaming my parents for not knowing about EDS. What am I hoping to do is encourage those of you diagnosed with EDS (and know there is a 50/50 chance that each of your children will inherit the gene for EDS) will consider the implications of the disorder. Please, if you suspect you child has EDS, do not push him/her if s/he is in pain. Whatever the sport is, your child's health is more important. Remember that for EDS patients, the damage caused now is long-lasting. Local anaesthetic failure in joint hypermobility syndrome
Summary: When taking biopsies to assess skin strength in Ehlers–Danlos syndrome type III (EDS–III), a Danish group noticed that the patients experienced much pain despite conventional local anaesthesia. When asked, all these patients reported previous experience of partial or complete failure of local anaesthesia in dental or obstetric procedures—for which reason some had been dismissed as hysterics. Pursuing this finding, Arendt-Nielsen compared the effects of local anaesthesia in 8 patients with EDS–III and 8 controls. Although the patients did gain analgesia from intradermal lidocaine the duration of effect was much shorter than in controls. EDS–III (now known as EDS–hypermobility type) is regarded by many authorities as identical to joint hypermobility syndrome (JHS). We wish to draw attention to the possibility of resistance to local anaesthesia in individuals with this common and under-diagnosed condition. Although the pathophysiology of this phenomenon remains unresolved, an important clue that a patient is at risk of local anaesthetic failure might be in front of our eyes. Full text here. | Amie K.EDS warrior. Find me on Twitter and Inspire as LilacZebra. Questions, comments, and/or suggestions? Email me ArchivesCategoriesAll |
 RSS Feed
RSS Feed